The Pregnancy Cancer Connection
This was an article written in 2012 printed in Positive Health online magazine.
It is really a concept introduction for lay people and health professionals to understand the similarities between cancer and pregnancy mechanisms. All still useful ideas.
Read the new piece on
to get another viewpoint.
The Pregnancy Cancer Connection

Hypomethylation
v's Hypermethylation of DNA in Cancer
It is really a concept introduction for lay people and health professionals to understand the similarities between cancer and pregnancy mechanisms. All still useful ideas.
Read the new piece on
to get another viewpoint.
The Pregnancy Cancer Connection
The pregnancy link with cancer goes back to John Beard in
1902 who wrote about The
Action of Trypsin[1] coming from the foetal pancreas to act on
switching off trophoblast function. Trophoblasts are cells that surround the
embryo and then form the umbilical cord which grows and creates an entire new
set of arteries between mother and child, using the placenta as an organ for
transferring maternal-foetal gas, nutrients and waste products.
The blood from the child and mother do not mix, as that
can set off an immune reaction so the oxygenated blood from the mother passes
the nutrients needed via a thin membrane called the syncytiotrophoblast. To do
all of this, arteries and collagen have to be remodelled in the mother to allow
40% of the mother's blood to feed the baby.
The numbers go like this "At term, maternal blood
flow to the placenta is approximately 600-700 ml/minute.
It is estimated that the surface area of syncytiotrophoblasts
is approximately 12m2 and the length of foetal capillaries of a
fully developed placenta is approximately 320 kilometres at term"[2] which
is an enormous amount of arterial remodelling to divert blood to the foetus.

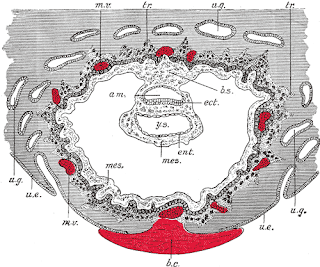
Section through
ovum imbedded in the uterine decidua. Semidiagrammatic. (After Peters.) am.
Amniotic cavity. b.c. Blood-clot. b.s. Body-stalk. ect. Embryonic ectoderm.
ent. Entoderm. mes. Mesoderm. m.v. Maternal vessels. tr. Trophoblast. u.e.
Uterine epithelium. u.g. Uterine glands. y.s. Yolk-sac.
This image is in
the public domain
because its copyright has expired. This applies worldwide
Beard noticed that when the pancreas began working in a
foetus around the 56th day, the pancreas began helping to breakdown hCG or
Human Chorionic Gonadotropin via enzymes, hence Beard used pancreatic enzymes
as a cancer cure. The 56th day I cannot confirm and hCG seems to maintain high
levels throughout the pregnancy.
The placenta and trophoblasts both release Human Chorionic
Gonadotropin as a hormone to maintain the corpus luteum which is like an egg
yolk left behind in the ovaries, the corpus luteum then releases the hormone
progesterone which signals to the uterus to thicken the endometrium or uterine
wall and sustain the zygote (the egg fertilized by sperm to become the embryo)
that has implanted itself into the uterine wall.
This is why progesterone is used to prevent pregnancy;
higher levels of progesterone convince the body it is pregnant and stop the
release of more eggs. I'll mention that progesterone only birth-control pills
have just had a study indicating depression in women using them.[3]
The placenta takes over from the corpus luteum to make
progesterone around 8 to 12 weeks, interestingly "progesterone
significantly upregulated the HERV-W env expression" HERV-W being the main
retrovirus active in the placenta; env is short for the retroviral envelope all
retroviruses have to enable cell fusion to occur.[4]
This is all related and I'll go into details later, the
Env of any of our retroviruses seem to cause problems as there is "the
potential of Env proteins to induce cell fusions, which may contribute to
tumour progression or even aid in metastasizing processes".[5]
The pregnancy test uses hCG as a marker and if not
pregnant can indicate reproductive or germ cell tumours so there is a strong
link with too much hCG and cancer; hCG has been used for years as an unproven
diet fix to reduce fat but the FDA stepped in to ban it in 2011.
John Beard[6] is still subject to controversy as you'll
find his theories attacked rather impolitely in Quackwatch because Dr Nicholas Gonzalez from the US recently
did studies used similar enzyme therapies on pancreatic cancer patients. You
can decide from Dr Gonzalez's list of case studies whether the enzymes
work;[6-7] meanwhile the orthodox approach is to make anti-hCG
vaccines.[8]
Putting aside biased opinions against natural therapies
controlling the trophoblastic actions of a tumour should be basic knowledge in
cancer treatment.

This image is in
the public domain
because its copyright has expired. This applies worldwide
There is also a long list of non-toxic foods and teas that
affect caspases and they are commonly used in alternative treatment of cancer,
though the practitioners may not be aware of their caspase properties. What is
as interesting are the similarities between embryonic implantation and tumour
attachment; both involve angiogenesis or new arterial growth and to do this
cells of the uterine wall and its collagen matrix have to be dismantled and
removed.
Trophoblasts create angiogenesis[12] to divert blood
supply and also release collagen destroying enzymes called metalloproteinases.
Tumours also create angiogenesis[13] to divert blood supply and release
collagen destroying enzymes called metalloproteinases.
A lot of studies use the trophoblast / tumour similarities
as a basis for cancer research; much of the research happened in the last
decade because before that the genomic elements like retroviruses that turn up
in the placenta and in tumours were seen as junk DNA or infections and cancer
research was geared towards affecting oncogenes (cancer promoting genes) and
tumour suppressor genes in our DNA.
After the Genome Project it was realized that between 8 to
10% of our DNA is made of retroviruses with retrotransposons or jumping genes
like Line1s, SINE1s and Alus bringing the level of jumping genes up to half of
our DNA so what did all this 'junk DNA' do?
Those retroviruses, oncogenes and tumour suppressor genes
all get affected by methylation which is like a chemical button called methyl
that binds to DNA to act as a DNA on / off switch. The Genome Project
discovered our DNA can be switched on and off by foods we eat and environmental
factors after birth and these changes to DNA affect cell functions and tumour
development so a new science developed quickly and has been called epigenetics.
Where We Are
It should be mentioned that cancer treatment theories fall
into alternative and orthodox ways of thinking and both are opposing camps of
thought with seemingly little dialogue between both camps. Alternative
therapies generally take the approach of detoxifying the body with the belief
that removing poisons and returning cells to a healthy state will stop tumour
growth.
Most alternative herbs and foods prevent attachment and
angiogenesis, some herbs have cytotoxic properties so I put them into a herbal
chemotherapy category. Alternatives can often take the stance that all orthodox
therapies are a no-go zone, when sometimes it may be appropriate to remove or
poison a tumour.
The other problem is good nutrients can unwittingly feed
tumour growth.
Mainstream medicine sees the tumour as something to remove
with surgery, poison with chemotherapy or radiate with radiation; all of these
approaches either remove the mass or try to kill the tumour. There is an
orthodox monopoly on treatment and this makes it impossible to really see what
other treatments may work on cancer, since most of the new orthodox drugs are
so new there is little evidence that they work in practice; otherwise there
would not be such a growing cancer epidemic with so many deaths.
The orthodox monopoly in itself may be a health hazard
because cancer interventions in my opinion are too rushed, the conditions for
cancer growth need to be managed first before surgery in particular. Cancer is
often said to be a "wound that does not heal", hence preparing the
body to heal wounds is necessary before possibly spreading tumour cells via
surgery.
Chemotherapy also only works while being taken; once
chemotherapy stops the same conditions for tumour growth can remain. The
mainstream also pays scant attention to the factors that lay the groundwork for
cancer growth so they have the philosophy that all of the body needs to be
carpet bombed by drugs. I think if dietary epigenetics was used to prevent
cancer spreading, then tumours could be individually targeted with drugs; this
would help avoid cancer patients dying from toxic organ failure due to the
cancer drugs.
In fact I think all of the chemotherapy is unnecessary,
because tumours can be injected with salt to kill them, this is because a
tumour is like an egg and shrivels up with salt, salt works by itself,[14] but
even more exciting is radiofrequency treatment which in effect cooks the tumour
like an egg plus salt injection to enhance the effect.
These were the results of salt injections combined with
radiofrequency treatment in a Chinese hospital treating liver cancer patients.
"The complete necrosis rate of tumours was 94%, and the necrosis rate of
tumours with diameter of 4.0 cm reached 100%."[15]
So both camps may not be aware of new research that
defines some very logical approaches that can go with both modes of thinking.
Here I will describe fascinating observations on tumours and pregnancy so this
is really a tour guide to send people to new places of thought.
"While on one hand, human placental cells are
bestowed with a capacity to proliferate indefinitely and invade extensively, on
the other, these cells are also replete with mechanisms to regulate these
tumour-like attributes and eventually progress to a senescent apoptotic state.
This is therefore, a 'well-behaved' tumour."[16]
"He was the first to point to the parallels between
cancer and the trophoblastic cells that envelop and nourish the embryo,
characterizing cancer as "irresponsible trophoblast."[17]
Immediately I expect to lose everyone's attention with the
word methylation but the "Hypomethylation v's Hypermethylation of DNA in
Cancer" question has had cancer researchers delving deep into these
epigenetic changes for years.[18]
Again genes get affected by methylation which is like a
chemical button called methyl that binds to DNA to act as a DNA on/off switch.
As an example the extremes of methylation in cancer have occupied researchers
for years.
"To date, a large amount of research on DNA
methylation and disease has focused on cancer and tumour suppressor genes.
Tumour suppressor genes are often silenced in cancer cells due to
hypermethylation. In contrast, the genomes of cancer cells have been shown to
be hypomethylated overall when compared to normal cells, with the exception of
hypermethylation events at genes involved in cell cycle regulation, tumour cell
invasion, DNA repair, and others events in which silencing propagates
metastasis."[19]
5-aza-2’-deoxycytidine or 5-aza-CdR is a standard
laboratory demethylating chemical for making genes switch back on again, so it
has been used in clinical trials on cancer patients in the hope tumour
suppressor genes would be turned on again and inhibit tumour growth.
Though in this study using 5-aza-CdR on breast cancer
cells they said it "draws attention to the potential danger in using
demethylating agents in anticancer therapy because of their potential effects
on activating a large number of quiescent genes including genes involved in
promoting tumour metastases. Nevertheless, it puts forward the opportunity of
an opposite approach, namely, inhibition of hypomethylation by hypermethylation
therapy"[20]
This is why I refer to laying the groundwork so
hypomethylation does not occur post surgery, because in the initial stages of
wound healing[21] as in foetal implantation the cells tend to be hypomethylated
or genes switched on. The safest and easiest way to address "inhibition of
hypomethylation by hypermethylation therapy" is the diet.
Some simplification of DNA may help understanding of these
processes.
When we are born we have an individual DNA chain that
decides a fair bit of blueprinting if you want to make the plan analogy.
Say each DNA base that make our genes is an equal sign =
and a chain of DNA stretched out is represented as a line of
===================== and is very long but twisted into a helical shape in
reality.
Epigenetics discovered the methyl groups are attached to
the genes or not, so a gene could methylated and silenced or unmethylated and
switched on. What we eat and environmental factors like chemicals, drugs and
radiation can change all the genes by switching some off and on. Cancer
theorists also have the 'Stem Cell Theory of Cancer"[22] which reasons
that some stem cells (the very first cell type) go wrong and can then become
cancerous, since stem cells appear in wounds and cancer, it has logic.
The exciting part of stem cell research has been
discovering stem cells can be obtained from either embryos but even better
taken from any person, cultured and then used to create new cells in the person
if say their nerve channels are broken.They also discovered the basic stem
cells from a person can be grown into any type of cell needed.
Different methylation profiles change stem cells into
specialised cells in our body, ones that go in different organs, cell layers
etc.
Say + is a methyl group to keep a gene quiet.
And Y is an unmethylated gene and switched on.
You start with the DNA chain of the stem cell as a
groundplan ======================
With methylated and unmethylated genes to decide cell
types +YYY+Y+++YYY+YY++Y+
This is from a stem cell study "Notably, even though
the iPS (Induced pluripotent stem) cells are derived from fibroblasts, their
R-DMRs (reprogrammed cells) can distinguish between normal brain, liver and
spleen cells and between colon cancer and normal colon cells. Thus, many DMRs
(differentially methylated regions) are broadly involved in tissue
differentiation, epigenetic reprogramming and cancer."[23
This is the answer to the hypomethylation versus
hypermethylation question; you need it all balanced to allow a cell to grow
into the right type of cell. If the differentially methylated regions get
muddled that is a big part of how a cancer starts. If your diet is low in
Folate, B12, B6, Selenium, Choline and a few other nutrients the genes can lose
the methyl group. This is how diet affects cancer growth, wound healing and
pregnancy. If you have too much Folate, B12, B6, Selenium, Methionine and
Choline in particular when pregnant some genes may not switch on.
If your diet is low in Vitamin A the genes can also get
switched off hence Retinoic acid, a form of Vitamin A gets used and works quite
well on cancers, in particular leukaemia and is a natural demethylating agent
that is a cell growth hormone.
Hence Vitamin A is vital for a proper pregnancy along with
Folate, B12, B6, Selenium, Methionine and Choline, but too much Vitamin A
switches on genes and can cause birth defects, Vitamin A is also great for
wound healing, the safest topical one is using rosehip oil.
Under extreme diet changes or exposure to drugs and
chemicals people lose all of the methyl groups and genes hypomethylate.
YYYYYYYYYYYYYYYYYYYYYYYYYYYYYYYYYYYYYY all on...
When all the genes switch on the stem cells can turn into
trophoblast type cells.
These trophoblast cell types can then express the same
retroviruses we see in cancer and pregnancy and create angiogenesis or new
arterial formation, collagen can get damaged in the process; it seems also an
underlying cause of all autoimmune diseases.
"Mouse embryonic stem cells can differentiate into
all three germ layers of the embryo but are generally excluded from the
trophoblast lineage. Here we show that ES cells deficient in DNA methylation
can differentiate efficiently into trophoblast derivatives."[24]
This is so important if stem cells revert to trophoblast
types, from a study clearly named 'DNA Methylation Changes in Sera of Women in
Early Pregnancy Are Similar to Those in Advanced Breast Cancer Patients' they
describe what the trophoblast type cells can do.
"In normal human pregnancy, the uterus and its
arterial system, including the decidua and the adjacent third of the
myometrium, are invaded by cytotrophoblasts, which initiate conversion of the
decidual vascular system from a high-pressure / low-flow system to a
low-pressure / high-flow system that meets the needs of the foetus and
placenta. The trophoblastic invasion in humans occurs between weeks 8 and 18 of
pregnancy. The invasion process into the uterus shows many similarities to the
invasion of malignant cells during metastasis in that both types of cells have
to pass through a basal membrane."[25]
Adequate levels of Vitamin D are also needed for cell
differentiation, this means Vitamin D can help cancer or trophoblast type cells
revert back to normal cell types and grow into mature normal cells. I can't
help but observe the plant analogy that Vitamin D from sunlight may guide our
cells.
“These observations suggest that non-toxic agents such as
retinoids (Vitamin A) and vitamin D, which have the ability to inhibit growth,
induce differentiation, inhibit vimentin expression, reduce cell motility,
inhibit uPA and MMP activity, and inhibit invasion and angiogenesis, are
potential cancer prevention and intervention agents.”
“These findings are significant, because vitamin D and
retinoids are both important chemopreventive agents and their combined use
permits a significant increase in drug efficacy at lower doses, thus
eliminating the risk of toxicity.”[26] Professionals need to be aware of this
if patients are inside and away from sunlight in hospitals and anyone with
darker skin is at even higher risk of Vitamin D deficiency. Without Vitamin D
the immune system will also fail.
“Activated vitamin D regulates the differentiation of stem
cells into monocyte and macrophage immune cells.”[27]
Inflammation, Cell Growth, Retroviruses and Cell to Cell
Fusion
"During tissue injury associated with wounding, cell
proliferation is enhanced while the tissue regenerates; proliferation and
inflammation subside after the assaulting agent is removed or the repair
completed. In contrast, proliferating cells that sustain DNA damage and / or
mutagenic assault (for example, initiated cells) continue to proliferate in
microenvironments rich in inflammatory cells and growth / survival factors that
support their growth. In a sense, tumours act as wounds that fail to
heal."[28]
Wound repair is a complex process involving blood factors,
immune white blood cells like neutrophils appear first and send out inflammatory
cytokines or signalling molecules, while white blood cells like macrophages
react to the inflammatory signals and appear on the scene to remove dead cells
and at the same time release growth factors.
The immune system generally deals with our own garbage
removal more than infections, hence buying shopping trolleys worth of soft
drinks or eating foods that clog up the system can predispose the body to
immune failure because it needs to deal with the garbage and if any pathogens
like bacteria, fungus and parasites get into the system they live off the
garbage while the immune system then has to deal with the overload.
This explains the basic philosophy of alternative
approaches which concentrate on toxin removal as part of cancer therapy. Our
own immune system is also the source of most inflammation so of course getting
the rubbish out of the way to calm down our white blood cells is going to avoid
repeated release of inflammatory cytokines and growth factors from white blood
cells.
When any cell growth happens retroviruses are involved in
the process this is why reverse transcriptase the particular enzyme
retroviruses use to replicate appears with cell growth.
"Expression of Reverse Transcriptase-coding genes is
generally repressed in non-pathological, terminally differentiated cells, but
is active in early embryos, germ cells, embryo and tumour tissues, all of which
have a high proliferative potential."[29]
When they say "terminally differentiated cells"
they mean cells that have matured and have their identities worked out. In
"early embryos, germ cells, embryo and tumour tissues" though there
is retroviral activity going on and exactly the sort of lowered methylation
that makes these cells potentially turn towards the trophoblast phenotype.
They also experimented with antiretroviral Nevirapine on
these cells and stopped them growing as well as rewriting gene expression so
stopping retroviruses will change your genes.
"Reverse Transcriptase inhibition induced an
extensive reprogramming of the gene expression profile both in cultured cell
lines and in preimplantation embryos."
Recent studies are showing embryonic stem cells have
retroviral activity so may be part of the gene switching mechanisms.[30-31]
Trophoblast cells in pregnancy have enormous retroviral activity in the form of
HERV-W or syncytin which also appears in breast and reproductive tumours along
with retroviruses like HERV-K which seems to appear in most tumours.
Syncytin is named after syncytium; this is where single
cells multinucleate or cluster together to make our organs and cell layers.
HERV-W or syncytin is creating cell fusion so gathering cells together. There
are 2 types of syncytin retrovirus: one seems to gather cells together while
the other affects the remodelling.
"Overexpression of different human endogenous
retroviruses (HERVs) has been shown in stem cell tumours, melanomas, human
embryonic stem cells as well as in the placenta. The envelope proteins of
HERV-W (also known as syncytin 1) and HERV-FRD (syncytin 2) were shown to be involved
in cell fusion allowing to generate the syncytiotrophoblast in the human
placenta. One of them, syncytin 2, was shown to be immunosuppressive, the
immunosuppressive activity was associated with its immunosuppressive (isu)
domain. Here we report the expression of another HERV, HERV-K..."[32]
Both HERV-FRD (syncytin 2) and HERV-K are
immunosuppressive because the immune system sees them as necessary. If HERV-W
or HERV-FRD are not expressing this is a big risk factor for preeclampsia,
because without these retroviruses working the blood supply and arterial
remodelling does not happen as well and this reduces nutrients to the
foetus.[33]
So the retroviruses in pregnancy are vital for cell
fusions to occur, but in a tumour this needs to be stopped. Cell fusions by
retroviruses apart from pregnancy also create multinucleate cells where single
cells in our body are fused together.
This is so new the research has to speak for itself.
There are "cell-cell fusions in connection with human
endogenous retroviruses (HERV ) in cancer. Examples of multinucleated cells
presented include placental syncytiotrophoblasts, muscle myotubes, bone
osteoclasts involved in normal human development and cell-cell fusions detected
in tumours. Examples of multinucleated cells in various cancers include germ
cell tumours, glioblastoma, melanoma, lung, breast, ovarian and endometrial
carcinomas."[34]
"deregulation of physiological fusogenic proteins in
tumour cells may promote cell fusion. For example, syncytin, the Env protein of
HERV-W human endogenous retroviruses and putative mediator of trophoblast
fusion, was also found to mediate fusion between breast cancer cells and
endothelial cells. CD44, a cell surface receptor known to be involved in cell
fusion during osteoclastogenesis, is frequently over-expressed in cancer cells
and has been linked to poor prognosis and cancer stem cell phenotypes."
"chronic inflammation has recently been shown to
dramatically increase the frequency of cell fusion between hematopoietic cells
(blood cells) and various somatic cells such as cardiomyocytes, skeletal
muscle, hepatocytes, and Purkinje cells during tissue repair and regeneration.
Similar as-yet-unknown mechanisms underlying this observation may also
stimulate the fusion between bone marrow-derived cells (BMDC) and tumour cells,
because inflammation is often associated with the tumour
microenvironment."
"and cell fusion may be the by-product of
“cell-eat-cell” processes, such as phagocytosis of tumour cells by macrophages
or entosis".[35]
Though the immune system is a tricky problem in cancer.
The trophoblast cells in pregnancy express what I call the
"this is a baby leave it alone" marker or self antigen HLA-G.[36]
Human leukocyte antigens on cell surfaces or HLAs are involved in letting the
immune system know this is a self-cell and not foreign to the body. Any
mutations or damage to HLAs are a big part of autoimmune disease causation as
the immune system can get confused and attack our own cells. During pregnancy
the immune system sees HLA-G and leaves trophoblast cells alone to do their
work.
"Isoforms of HLA-G saturate the maternal-foetal
interface and circulate in mothers throughout pregnancy. Uteroplacental immune
privilege for the foetus and its associated tissues is believed to result when
immune cells encounter HLA-G."[37]
The problem with tumours is they also express HLA-G
antigens just like trophoblast cells do.
"Convincing clinical evidence indicates that the
limited success of T-cell-based immunotherapy of malignant diseases is caused,
at least in part, by the ability of malignant cells to escape from immune
recognition and destruction. Among the multiple escape mechanisms identified, a
major role is played by changes in the expression and/or function of HLA
antigens expressed by tumour cells, because they may markedly affect tumour
cell-host's immune system interactions."[38]
Boosting the immune system in fact can have the complete
opposite effect, it can spread the tumour. This is important to know for
alternative practitioners who may use things like Echinacea and Astragalus to
boost T-cells.
"As the immune surveillance is not sufficient
anymore, tumour-associated macrophages contribute to tumour progression. It is
notable that tumour-associated macrophages promote the proliferation of tumour
cells directly by secreting growth factors. They also participate in tumour
progression by acting on endothelial cells and thus promoting the
neovascularization of the tumour. Tumour-associated macrophages are indeed key
protagonists during angiogenesis and promote each step of the angiogenesis
cascade."[39]
Cell fusions and retroviruses may actually contribute to
this process, if tumours are releasing retroviral envelopes then it is quite
likely the tumours could be binding macrophages to their edges and using
macrophages to burn new arterial channels[40] as this seems to be the case
during pregnancy.[41]
"Decidual artery remodelling is essential for a
healthy pregnancy."
"In early stages of remodelling, vascular smooth
muscle cells showed dramatic disruption and disorganization before vEVT
(endovascular trophoblasts) presence. Leukocytes (identified as uterine natural
killer cells and macrophages) were apparent infiltrating vascular smooth muscle
cells layers and were matrix metalloproteinase-7 and -9
immunopositive."[42]
"matrix metalloproteinase-7 and -9" are collagen
destroying enzymes that tumours also produce. The cell fusions that occur may
mean the tumours bind to our own macrophages. The reason for normal macrophage
cell fusion is described here; it means that when infections from viruses,
bacteria, fungi, parasites, chemical or radiation exposure or literally
anything that damages cells so the dead cells or pathogens need removing may be
accompanied by retroviral activity to fuse macrophages into bigger
multinucleate cells to do the job.
"Cells of the mammalian monocyte-macrophage lineage
form two major types of multinucleated cells: macrophage giant cells in many
tissues and osteoclasts in bone. In each case, the physiological roles of these
cells involves endocytosis and resorption of relatively large objects,
including cell corpses, invading pathogens, foreign bodies, and chunks of
mineralized bone. The increased size achieved through cell fusion presumably
affords the extra membrane surface area and endosome / lysosome volume to
achieve these tasks. In addition, it is conceivable that a larger cell can more
safely distance the nuclei and cell body from the noxious degradative cocktails
used to dispose of objects within the engulfment apparatus."[43]
A French study asked this very question?
"Macrophages recognize each other as self in
order to fuse but some essential questions remain: do macrophages fuse with
somatic cells to repair tissues and organs? Do macrophages fuse with tumour
cells to trigger metastasis?"[44]
Going Back A Century
Cancer is now an epidemic disease, rates nearing one in
two. Living longer is a factor but things have changed: we have high-tech
medical interventions, vaccines, new drugs, hormone drugs, new chemicals, pesticides,
trans fats and GMOs in food, new radiation sources from our electronics, less
sunlight, less exercise.
Wealthier people are eating more meat, more sugar, alcohol
is massively consumed as always; by the time someone turns up to the hospital
with a tumour it's impossible to know what caused it. In poorer countries they
suffer cancers from reckless industrial pollution while going to work can be a
chemical hazard. Since the financial collapse, the water and sewage
infrastructure of many countries went backwards so cancers from pathogens are
also in the mix. The attitude to cancer in itself lends to voodoo, if you tell
people they will die they will die.
I've been amazed at personal stories told where a patient
had surgery and chemotherapy and been dead in less than 2 months and I've
witnessed others. Our obsession with expensive cancer interventions may be a
terrible waste of tax payers’ money while emergency rooms can't even be funded.
My dad for instance has had surface tumours for 30 years, he has avoided doctors and kept it simple and cheap by making his own salt bags or pads to apply heated salt while sleeping overnight. There are clear studies saying salt injected into tumours works so my dad's intuitive approach seems to work too.
So in my opinion people with cancer have time; if you can walk perhaps it is healthier to take a holiday first, change your diet and get a bit of fresh air and then come prepared for treatment. Most of our cancers are life-style related, so taking your mind and body somewhere else is a possible road to a cure.
My dad for instance has had surface tumours for 30 years, he has avoided doctors and kept it simple and cheap by making his own salt bags or pads to apply heated salt while sleeping overnight. There are clear studies saying salt injected into tumours works so my dad's intuitive approach seems to work too.
So in my opinion people with cancer have time; if you can walk perhaps it is healthier to take a holiday first, change your diet and get a bit of fresh air and then come prepared for treatment. Most of our cancers are life-style related, so taking your mind and body somewhere else is a possible road to a cure.
To sum up my thoughts on treatment, anti-inflammatory
foods work. Red meats and dairy are actually inflammatory due to a Sialic acid
they contain which is foreign to humans, we are mildly allergic to all mammals
but not fish, birds or reptiles so any red meats can cause long term
inflammation. The Sialic acid from dairy foods can also feed tumours and I
suspect the same with eggs and they are both baby foods so avoid them in
excess. Phytates or IP6 from legumes, seeds, grains and bran may chelate
minerals but inhibits cancer.
Iron is inflammatory and feeds cancer as well as
infections. The nutrients needed for methylation can also affect Iron
absorption, to absorb Iron so it is used by the blood and does not become inflammatory
we need Folate, B12, B6, Copper and Vitamin C in our diet. Folate, B12, B6,
Selenium, methionine, Choline along with Vitamin A and D are needed to balance
methylation.
Genetically anyone with mutations to Folate processing
genes MTHFR1 and C677T need to be aware this can cause long term
hypomethylation and dispose them to trophoblast type cells.
This is where genetic testing can prevent cancers; they
can work out methylation levels in people before it becomes a problem. Folate
supplementation can encourage cancer growth though hence the need to know if
you have problems with those genes. Too much Iron also can affect Selenium
levels and the thyroid needs Selenium.
Thyroid hormones encourage both trophoblast and tumour
invasion, and a lack of Selenium can cause hyperthyroid and wasting or
cachexia. While Iodine without Selenium makes more thyroid hormones,
hence Iodine deficiency is also a risk for pregnancy loss because the
trophoblasts need thyroid hormones to work.
Since tumours dissolve collagen Lysine tablets or foods
with Vitamin C to remake collagen are part of the anti-angiogenesis formula.
Proanthocyanidins from berries, Resveratol from grapes, Carotenoids from all
the yellow / orange/red veggies have effect.
Green tea, Turmeric and Oleuropein from olives are potent
anticancer compounds and anti-inflammatory. Green tea even works better at
preventing tumour attachment with Vitamin A.
My favourite anticancer compound is Bromelain, I use it to
fix psoriasis. It is one of the best anti-inflammatory chemicals around, it
breaks up fibrin and can be used as a blood thinner though any signs of
bleeding stop using it. If Bromelain can be used it will prevent tumour
attachment to CD44 molecules and also inhibits the inflammatory cytokines.
CD44 is also used for trophoblast attachment so don't take
Bromelain if pregnant.
I want to see the study on what Bromelain does to
retroviruses like HERV-W and HERV-K, waiting for that one.
Every one of the food chemicals above from Selenium to
Bromelain also affect Caspase enzymes so tell tumours to stop.
These ideas can be researched and used by anyone including
people using chemotherapy.
Bromelain for instance actually potentiate drugs.
Doctors using chemotherapy should be using detection scans
to target chemotherapy directly to tumours and not all of the body, while being
aware they can use all of the above.
I recommend reading Nutrition and cancer: A review of the evidence for an
anti-cancer diet by Michael S Donaldson[45] and the book Natural compounds in cancer therapy
by John Boik [46] and Nutrition
and Cancer State of the Art by Sandra Goodman PhD[47]as a start for
further research; they are available online.
References
1. Beard J. The Action of Trypsin. British Medical
Journal. 4:140-41. 1906.
2. Wang Y & Zhao S. Vascular Biology of the Placenta.
San Rafael (CA): Morgan & Claypool Life Sciences 2010.
3. Girdler SSet al. A history of depression in women is
associated with an altered GABAergic neuroactive steroid profile.
Psychoneuroendocrinology. 37(4):543-5. April 2012.
4. Noorali S et al. Role of HERV-W syncytin-1 in
placentation and maintenance of human pregnancy. Applied Immunohistochemistry
& Molecular Morphology. 17(4):319-28. July 2009.
5. Mullins CS & Linnebacher M. Human endogenous
retroviruses and cancer: Causality and therapeutic possibilities. World Journal
of Gastroenterology. 18(42): 6027–6035. November 2012.
6. Beard J. The Enzyme Treatment of Cancer. London: Chatto
and Windus. 1911.
7. Nicholas J. Gonzalez NJ & Isaacs LL. The Gonzaez
Therapy and Cancer: A Collection of Case Reports. Alternative Therapies. Vol
13. No. 1. Jan/Feb 2007.
8. Delves PJ et al. Designing a new generation of anti-hCG
vaccines for cancer therapy. Molecular Cell Endocrinology. 2;260-262:276-81.
January 2007.
9. Longtine MS et al. Caspase-mediated apoptosis of
trophoblasts in term human placental villi is restricted to cytotrophoblasts
and absent from the multinucleated syncytiotrophoblast. Reproduction.
143(1):107-21. January 2012.
10. Olsson M & Zhivotovsky B. Caspases and Cancer.
Cell Death & Differentiation. 18(9):1441-9. September 2011.
11. Ofir R et al. Taxol-induced apoptosis in human SKOV3
ovarian and MCF7 breast carcinoma cells is caspase-3 and caspase-9 independent.
Cell Death & Differentiation. 9 (6):636-642. June 2002.
12. Lash GE et al. Secretion of angiogenic growth factors
by villous cytotrophoblast and extravillous trophoblast in early human
pregnancy. Placenta. 31(6):545-8. June 2010.
13. Weis SM et al. Tumour angiogenesis: molecular pathways
and therapeutic targets. Nature Medicine. Vol. 17:1359–1370.. November 2011.
14. Lin YC et al. Ablation of liver tumour by injection of
hypertonic saline. American Journal Roentgenology. 184 (1):212-9. January 2005.
15. Feng G et al. Hypertonic saline enhanced
radiofrequency ablation in the treatment of liver cancer. Chinese Journal of
Digestive Surgery. 8 (2):110-112. 2009.
16. Soundararajan R & Rao AJ. Trophoblast
'pseudo-tumourigenesis': Significance and contributory factors. Reproductive
Biology and Endocrinology. 2:15. 2004.
17. Moss RW. The life and times of John Beard, DSc
(1858-1924). Integrated Cancer Therapies. 7(4):229-51. December 2008.
18. Ehrlich M. DNA methylation in cancer: too much, but
also too little. Oncogene. 21:5400-5413. 2002.
19. Phillips T. The role of methylation in gene
expression. Nature Education 1(1). 2008.
20. Ateeq B et al. Pharmacological Inhibition of DNA
Methylation Induces Proinvasive and Prometastatic Genes In Vitro and In Vivo.
Neoplasia. 10(3): 266–278. March 2008.
21. Arwert EN et al. Epithelial stem cells, wound healing
and cancer. Nature Reviews Cancer. 12(3):170-80. February 2012.
22. Gil J et al. Cancer stem cells: the theory and
perspectives in cancer therapy. Journal of Applied Genetics. 49(2):193-9. 2008.
23. Doi A et al. Differential methylation of tissue- and
cancer-specific CpG island shores distinguishes human induced pluripotent stem
cells, embryonic stem cells and fibroblasts. Nature Genetics. 41(12):1350-3.
December 2009.
24. Ng RK et al. Epigenetic restriction of embryonic cell
lineage fate by methylation of Elf5. Nature Cell Biology. 10(11):1280-90.
November 2008.
25. Müller HM et al. DNA Methylation Changes in Sera of
Women in Early Pregnancy Are Similar to Those in Advanced Breast Cancer
Patients. Clinical Chemistry. 50 (6): 1065-1068. June 2004.
26. Tokar EJ et al. Retinoids, vitamin D, invasion, and
metastasis. Current Oncology. 13(6): 198–200. December 2006.
27. Arnson Y et al. Vitamin D deficiency is associated
with poor outcomes and increased mortality in severely ill patients. Quarterly
Journal of Medicine. doi:10.1093/qjmed/hcs014. February 2012.
28. Coussen LM & Werb Z. Inflammation and cancer.
Nature. 420(6917): 860–867. Deccember 2002.
29. Spadafora C. Endogenous reverse transcriptase: a
mediator of cell proliferation and differentiation. Cytogenetic Genome
Research. 105(2-4):346-50. 2004.
30. Macfarlan TS et al. Embryonic stem cell potency
fluctuates with endogenous retrovirus activity. Nature. 5;487(7405):57-63. July
2012.
31. Kunarso G et al. Transposable elements have rewired
the core regulatory network of human embryonic stem cells. Nature Genetics.
42:631–634. 2010.
32. Kammerer U et al. Human endogenous retrovirus K
(HERV-K) is expressed in villous and extravillous cytotrophoblast cells of the
human placenta. Journal of Reproductive Immunology. 91(1-2):1-8. September
2011.
33. Vargas A et al. Reduced Expression of Both Syncytin 1
and Syncytin 2 Correlates With Severity of Preeclampsia. Reproductive Sciences.
18 (11) 1085-1091. November 2011.
34. Strick R et al. Cell–Cell Fusions and Human Endogenous
Retroviruses in Cancer. Cell Fusions. pp 395-426. 2011.
35. Lu X. & Kang Y. Cell Fusion as a Hidden Force in
Tumour Progression. Cancer Research. 69:8536-8539. November 2009.
36. Rizzo R et al. The importance of HLA-G expression in
embryos, trophoblast cells, and embryonic stem cells. Cellular and Molecular
Life Sciences. 68( 3):341-352. February 2011.
37. Hunt JS et al. The role of HLA-G in human pregnancy.
Reproductive Biology and Endocrinology. 4 Suppl 1:S10. 2006.
38. Rouas-Freiss N et al. HLA-G Proteins in Cancer: Do
They Provide Tumour Cells with an Escape Mechanism. Cancer Research. 65; 10139.
November 2005.
39. Lamagna C et al. Dual role of macrophages in tumour
growth and angiogenesis. Journal of Leukocyte Biology. 80(4):705-713. October
2006.
40. Shih J et al. Tumour-Associated Macrophage: Its Role
in Cancer Invasion and Metastasis. Journal of Cancer Molecules. 2(3) p. 101.
2006.
41. Whitley GStJ. & Cartwright JE. Cellular and
Molecular Regulation of Spiral Artery Remodelling: Lessons from the
Cardiovascular Field. Placenta. 31(6): 465–474. June 2010.
42. Smith SD et al. Evidence for Immune Cell Involvement
in Decidual Spiral Arteriole Remodeling in Early Human Pregnancy. American
Journal of Pathology. 174(5): 1959–1971. May 2009.
43. Mohleer WA. Cell-Cell Fusion: Transient Channels
Leading to Plasma Membrane Merger. Madame Curie Bioscience Database [Internet]
Austin (TX): Landes Bioscience. 2000.
44. Vignery A. La fusion des macrophages: partenaires des
cellules somatiques et cancéreuses? Medecine Sciences. 21(12)p.1070-1075.
December 2005.
45. Donaldson M. Nutrition and cancer: A review of the
evidence for an anti-cancer diet. Nutrition Journal. 3:19. 2004.
46. Boik J. Natural compounds in cancer therapy. Oregon
Medical Press. 2001.
47. Goodman S. Nutrition and Cancer: State-of-the-Art.
Green Library. 1995; Positive Health Publications Ltd. 1998; Health Research
2003. www.drsgoodman.com/books-goodman/52-nutrition-and-cancer[1] [2]


{kind=link}
{kind=link}
Comments
Post a Comment